Indications:
- Symptomatic or unstable bradycardia / AV Block
- Severe sick sinus syndrome with prolonged asystole (>3 seconds) and syncope
- Ventricular standstill due to complete heart block or Mobitz type II AV block
- Torsades de pointes (Overdrive pacing)
- Recurrent monomorphic ventricular tachycardia (Over drive pacing); risk of inducing Vfib
- Unstably SVT – only after pharmacologic intervention and cardioversion has failed
Preferred sites:
- Right internal jugular vein
- Left subclavian vein
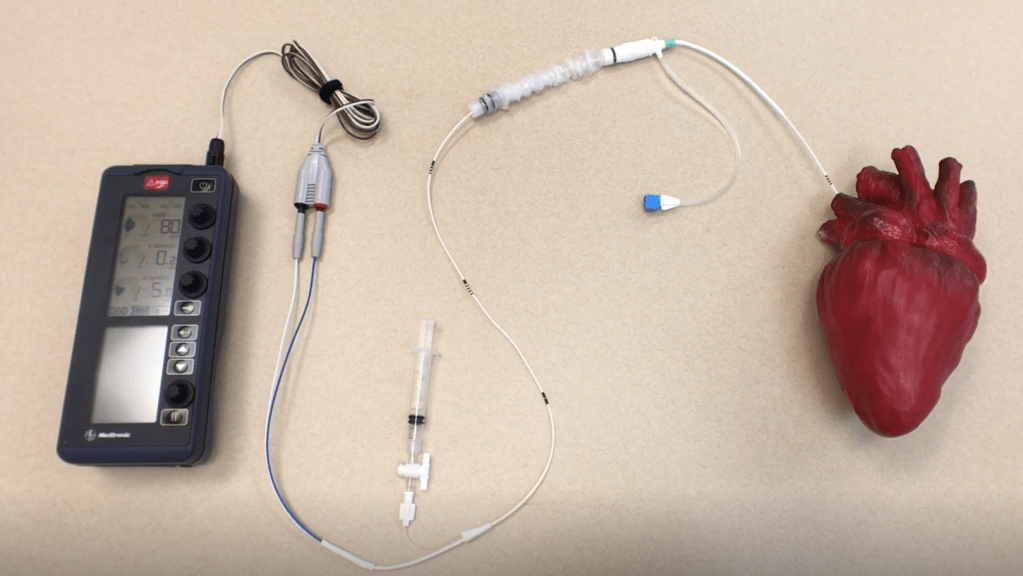
Procedure:
- Place cordis
- Have an assistant plug the non-sterile side of the connecting cable into the generator
- Confirm balloon inflates using the 1cc syringe; leave it deflated
- Feed the wire through the smaller side of the sterile sleeve
- Feed the wire at least 20 cm (two black lines) into the cordis; this places the balloon just outside the cordis sheath
- Place the black adapter pins into the pacing wire and have an assistant plug them into the connecting wire (Negative to negative; positive to positive)
- Have assistant change rate to 80 bpm and set output to 20 mA
- Feed the wire 30 cm in (three black lines), and inflate and lock the inflated balloon
- Using a subxiphoid view of the right ventricle or watch the cardiac monitor for a STEMI pattern in lead I
- Once you have capture, turn down the current until you just lose capture, then go one above that
- Deflate the balloon and lock
- Pull the sleeve down to the cordis and open up the sterile sleeve
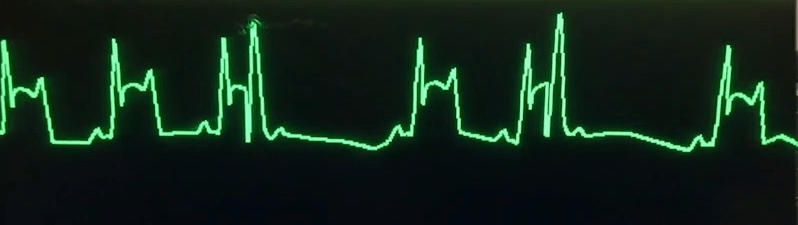
STEMI Pattern in Lead I
References

Leave a comment