Five common pitfalls:
- Over-reliance on symptoms quality (e.g. “spinning” v. “lightheadedness”)
- Underuse of timing and triggers
- Lack of familiarity with key physical exam findings
- Overweighing traditional risk factors (e.g. age, vascular risk factors)
- Over-reliance on CT
The “ATTEST” Diagnostic Paradigm – Associated symptoms, timing and triggers, exam findings, and additional testing (… see how nicely this acronym works)
Name of the game: Rule out dangerous causes by ruling in benign causes
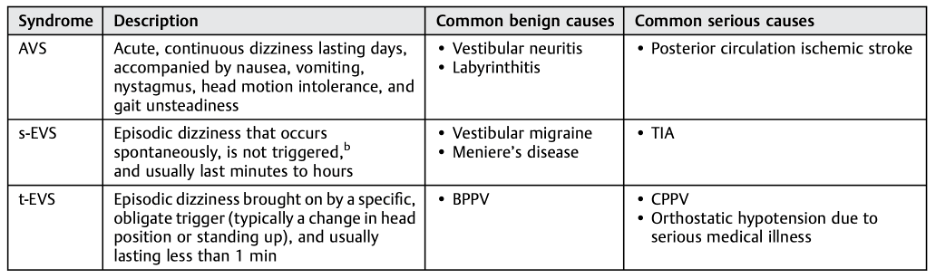
Identify which of the three syndromes best fits the dizziness described
Acute Vestibular Syndrome (AVS)
- Acute onset of persistent, continuous dizziness lasting >24 hours
- Associated with nausea, vomiting, nystagmus, gait instability, and head-motion intolerance
- Most common benign causes: Vestibular neuritis (dizziness only) and labyrinthitis (dizziness + hearing loss/tinnitus)
- Dangerous cause: Posterior circulation stroke
- GRACE-3 recommendation:
- Use the HINTS exam and test hearing in patients with nystagmus to differentiate a central from peripheral diagnosis
- Assess severity of gait unsteadiness in patients without nystagmus
- In patients whose HINTS result is central or equivocal, use MRI/MRA to distinguish between central and peripheral diagnoses
- CT cannot rule out acute ischemic stroke in AVS (Sensitivity of 7-16% in first 24 hours of onset)
Spontaneous Episodic Vestibular Syndromes (s-EVS)
- Recurrent (non-triggerable) episodes of dizziness that range in duration from seconds to days; majority of which lasts minutes to hours
- Diagnosis relies heavily on history and neuro exam; the HINTS exam may be helpful if the patient is actively dizzy
- Most common benign cause: Vestibular migraine
- Also consider Meniere’s Disease, vasovagal syncope, panic attacks; cardiovascular, endocrine, and toxic causes
- Most common dangerous cause: Posterior circulation TIA
- GRACE-3 recommendation:
- Do not use CT to distinguish between central and peripheral diagnoses
- If concern for TIA, use CTA or MRA to diagnose large vessel pathology
Triggered Episodic Vestibular Syndromes (t-EVS)
- Brief episodes of dizziness lasting seconds to minutes with an obligate trigger
- The patient must have a normal baseline
- Do not confuse exacerbating factors (makes baseline dizziness worse) with triggers (provokes new dizziness)
- Focus on the physical exam
- Most common benign causes: BPPV, orthostatic hypotension
- Most common dangerous causes: Neurologic mimics of BPPV (e.g. posterior fossa neoplasm, infarction, hemorrhage, or demyelination), dangerous causes for orthostatic hypotension
- GRACE-3 recommendation:
- Use the Dix-Hallpike test to diagnose posterior canal BPPV
- Do not routinely use CT or CTA
- For posterior canal BPPV by a positive Dix-Hallpike test, do not routinely use MRI or MRA
The HINTS Exam
- Horizontal head impulse testing (Head Impulse)
- Direction-changing nystagmus in eccentric gaze (Nystagmus)
- Vertical skew (Test of Skew)
A single central finding on any of the 3 components “rules-in” a posterior circulation stroke, and further testing/treatment is indicated. The HINTS exam was more sensitive than an MRI in the first 24 hours. Studies have shown sensitivity of the HINTS to be 96-100%, with specificity 96-98%.
- Horizontal head impulse testing (Head Impulse)
- Hold the patient’s head, allowing their mandible to rest and relax into your palms. Ask the patient to fixate on an object (ie, your nose). Then, quickly and gently move the patient’s head to the left or right and then back to the neutral position again.
- Central Finding: Absence of saccade (no large beats of nystagmus as the eyes “catch up” to re-fixate on examiner’s nose) is concerning.
2. Direction-changing nystagmus in eccentric gaze (Nystagmus)
- Central Finding: Any vertical nystagmus or horizontal nystagmus that changes direction with lateral gaze (“bidirectional nystagmus”) is concerning.
3. Vertical skew (Test of Skew)
- Cover one eye for several seconds and then uncover that eye quickly.
- Central Finding: Realigning of the eye vertically is concerning.
- This response may fatigue over serial exams during a short time period.

Leave a comment